

Tennessee’s Budget, Explained: Rural health is one of the clearest budget items to watch
Rural health is one of the clearest parts of Tennessee’s budget to watch because the consequences are not abstract. They show up in drive times, emergency rooms, clinic access, hospital finances
The Redemption Project Newsroom
Rural health is one of the clearest parts of Tennessee’s budget to watch because the consequences are not abstract. They show up in drive times, emergency rooms, clinic access, hospital finances and whether families can find care close to home.
Health care is one of the largest and most complicated parts of state government.
That makes it easy to talk about and hard to explain.
One person may say “health care” and mean TennCare. Another may mean rural hospitals. Another may mean uncompensated care, behavioral health, dental coverage, workforce training, public health, disability services or access to doctors.
Those are related issues. They are not the same issue.
That distinction matters when reading Tennessee’s budget.
Tennessee’s fiscal year 2026-27 budget document places health and social services in its own major section. That section includes TennCare, mental health and substance abuse services, the Department of Health, disability and aging, human services, children’s services and other health-related programs.
The budget record includes several rural health items that are specific enough for citizens to track.
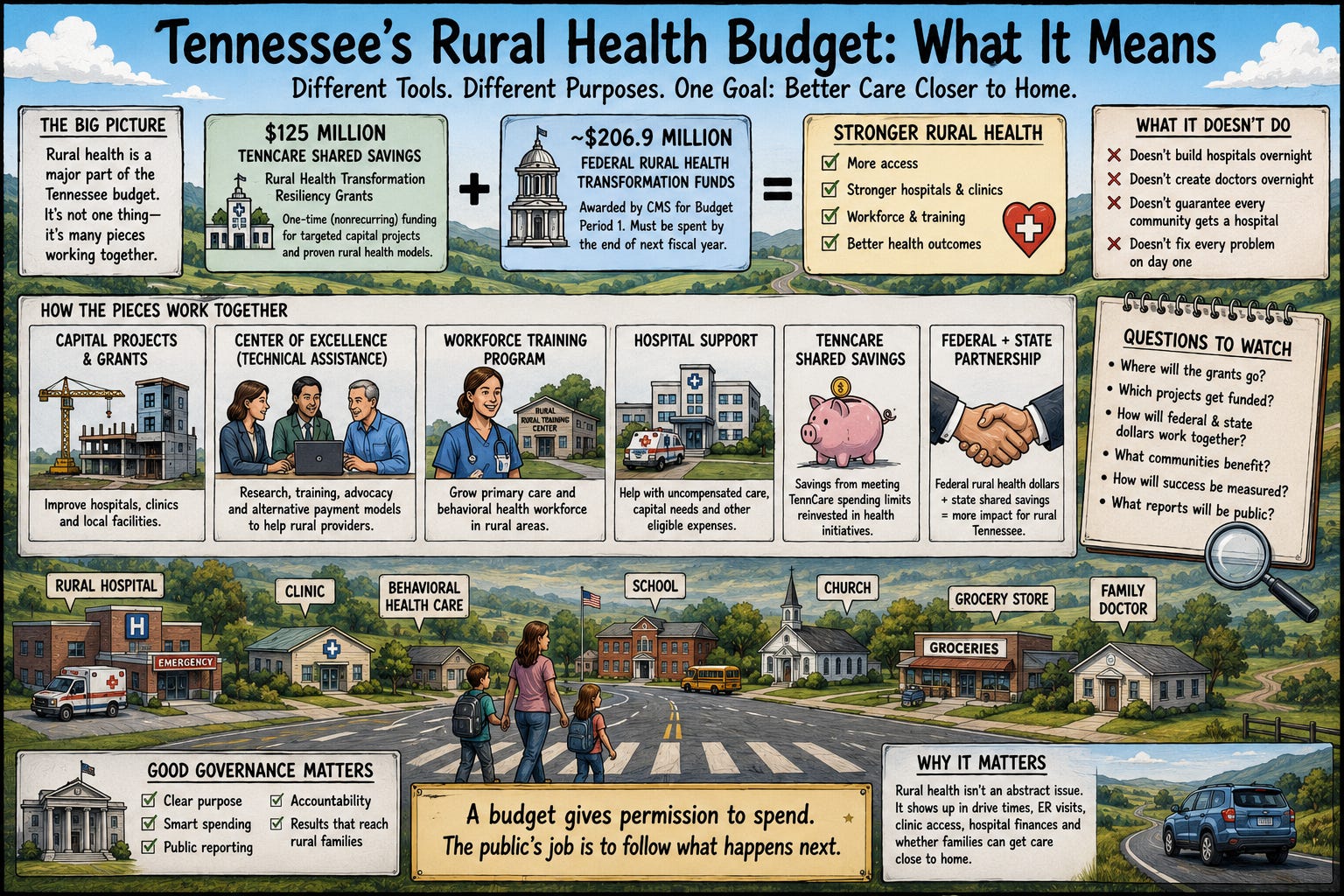
One of the clearest is $125 million in nonrecurring TennCare Shared Savings funding for Rural Health Transformation Resiliency Grants. The budget document says the funding is intended to supplement Tennessee’s federally funded Rural Health Transformation Program through targeted capital projects and to extend effective models emerging from that program.
That wording is important.
The $125 million is listed as nonrecurring. That means it is one-time funding, not an ongoing annual appropriation built into the base budget. It is also tied to TennCare Shared Savings, not described simply as ordinary General Fund spending.
The state’s Rural Health Transformation Program application uses similar language. It says Tennessee planned to invest $125 million in TennCare Shared Savings to strengthen rural health through targeted capital projects in hospitals and communities. The application describes those funds as matching or supplementing the federal rural health opportunity.
The Tennessee Department of Health says the Centers for Medicare and Medicaid Services awarded Tennessee approximately $206.9 million for Budget Period 1 through the federal Rural Health Transformation Program. The department says those funds are intended to support rural health transformation efforts and must be spent by the end of the next fiscal year.
That gives readers the basic structure.
There is federal rural health money. There is state TennCare Shared Savings money. The budget record identifies a $125 million nonrecurring state investment tied to rural health transformation. The Department of Health separately identifies approximately $206.9 million in federal Rural Health Transformation funding for Budget Period 1.
Those facts are important. They should not be overstated.
A budget appropriation does not guarantee that every rural community will have a hospital nearby. It does not create doctors, nurses, specialists or behavioral health providers overnight. It does not prove that rural hospital finances are stable long term.
What it does show is that rural health is not a side note in this budget record. It is specifically named, funded and connected to both state and federal health initiatives.
The budget document also lists additional rural health-related items using TennCare Shared Savings.
It identifies funding to continue a Center of Excellence for rural communities and providers. The stated purpose is technical assistance, research and advocacy to expand service delivery, evaluate alternative payment models and transition services to better meet rural community needs.
The document also lists funding for Center of Excellence grants and a Rural Health Care Training Program. The training program is described as addressing existing primary care and behavioral health workforce shortages in rural communities.
Those details matter because rural health is not only about buildings.
Capital projects can help hospitals and clinics. Training programs can address workforce needs. Technical assistance can help providers and communities adjust service models. Grants can support local implementation.
Those are different tools.
If voters hear only that Tennessee funded rural health, they may miss the more useful questions: Is the money for construction, workforce, grants, technical assistance or direct care? Is it state money or federal money? Is it recurring or one-time? Which agency administers it? Which communities receive it? What public reporting will show whether it worked?
The budget record also includes hospital-related funding described in legislative and media summaries.
WBIR reported that the budget included $137 million for hospitals, especially rural hospitals, to help cover uncompensated care, and $205 million in shared savings for health care initiatives, including rural health grants. Because that figure comes from a media summary of the legislative budget action, it should be attributed as reported unless matched directly to the budget document or adopted amendment.
That source distinction is not nitpicking.
It is how readers avoid confusion.
The budget document, adopted amendments, state agency materials, legislative summaries and media reports can all help explain the budget. But they are not the same kind of source. A careful reader should know whether a figure comes directly from the budget record or from a summary of the budget.
The rural health section is also a good reminder that health care funding often operates through layers.
TennCare is Tennessee’s Medicaid program. TennCare Shared Savings refers to savings Tennessee has received for meeting annual TennCare spending limits. The Sycamore Institute reported that Tennessee received $1.3 billion in shared savings between fiscal years 2023 and 2026.
Sycamore’s analysis was of the governor’s recommended fiscal year 2027 budget, so it should be used as context for the recommendation, not as a substitute for the final appropriations record.
The practical takeaway is simple: Tennessee’s health care budget is not one thing.
It includes TennCare. It includes rural health transformation. It includes federal funds. It includes state shared savings. It includes hospitals. It includes workforce training. It includes grants and technical assistance.
Each item needs to be read on its own terms.
For citizens, the real accountability comes after the budget passes.
Where will the Rural Health Transformation Resiliency Grants go? Which projects will receive funding? How will the federal and state rural health money interact? Which communities will benefit? Will the workforce training money reach rural areas with provider shortages? Will hospitals use support for capital needs, uncompensated care or other eligible purposes? What reports will show progress?
Those are not partisan questions.
They are stewardship questions.
A budget does not fix rural health care by announcing a number. It gives state government permission to spend money toward named purposes. The public’s job is to follow what happens next.
That is especially true for rural health, where the consequences are not abstract.
They show up in drive times, emergency rooms, clinic access, behavioral health availability, hospital balance sheets and whether families can find care close to home.
The budget record shows Tennessee put rural health money on the table.
The next question is whether that money reaches the places and problems it was meant to address.
I am a retired detective and criminal justice / government educator based in Tennessee. I am a commentary write for Tennessee Lookout and a weekly columnist with Knox TN Today. My work examines public policy, public safety systems and civic responsibility. My reporting and commentary have also appeared in Governing, The Arizona Capitol Times, South Florida Sun Sentinel, Police1, among other state and regional outlets.
